A pigment of imagination...
Racial superiority is a mere pigment of the imagination (author unknown)


We have an abundance of data with something to say. As an analyst I have been looking at structural determinants of health as the source of inequities. Look at the COVID-19 death rates by age and race. You have likely heard the adage that your zip code is a better predictor than your genetic code.

But why are these populations seeing the brunt of COVID-19? Because the gaps are absolutely huge — from age 35-44, Blacks die at a rate 10 times higher than whites. I think that most people here would agree that it’s not because there’s some fundamental difference between white and Black bodies — but rather that there are social differences that affect health outcomes: the stress of racism, history of housing discrimination, lack of equal access to healthcare, more exposure due to “frontline jobs”.
All of these risk factors and more are now lumped into a broad category called the social determinants of health, which the CDC defines are the conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks. — Anthony Breu, MD, podcast, The Original (Antigenic) Sin—Bedside Rounds
Many truths have been illuminated from the shadows of this global pandemic. My specific focus has been on race. The reason isn’t because I identify as black and white. The curiosity began when I was working as an emerging data analyst. In the beginning of my career, clients asked for specific metrics or demographic data to be included and I complied.
One day, I asked a client what the race data was going to represent. Today I would have specifically asked, “What data question are you attempting to answer.” I knew the variable was a poorly designed proxy for biology and at best was intended to serve as a political construct.
The answers were almost always consistent with, “Well, we always measure race.” Once I had the experience and skill to delve into large datasets like the US Census I began to see what the race variable was never intended or able to measure. When we look to measure equity—in my case—health equity, we need to look at a much larger infrastructure.
When we look closely at metrics compiled by Kaiser Family Foundation we can begin to see the complexity behind equity that extends far beyond skin color.
Economic Stability: employment, income, expenses, debt, medical bills
Neighborhood and physical environment: housing, transportation, safety, parks, playgrounds, walkability, zip code/geography
Education: literacy, language, early childhood education, vocational training, higher education, access to internet
Food: hunger, access to healthy options, distance from grocery store, food insecurity
Community and social context: social integration, support systems, community engagement, discrimination, stress
Health care system: health coverage, provider availability, provider linguistic and cultural competency, quality of care
Exploring racism in medicine or when we began bucketing folks into random categories goes back quite a long time.

Carl Linnaeus, father of taxonomy, also created a racial taxonomy based on the 4 humors; flegmat (phlegmatic), sangvin (sanguine), coleric (choleric), and melanc (melancholic).

The source of these distinctions inherited as far back as Aristotle, Hippocrates, and Galen originated from bodily humors; black bile, yellow bile, phlegm, and blood. An imbalance allegedly influenced your disposition.
●Americanus: red, choleric, righteous; black, straight, thick hair; stubborn, zealous, free; painting himself with red lines, and regulated by customs.
●Europeanus: white, sanguine, browny; with abundant, long hair; blue eyes; gentle, acute, inventive; covered with close vestments; and governed by laws.
●Asiaticus: yellow, melancholic, stiff; black hair, dark eyes; severe, haughty, greedy; covered with loose clothing; and ruled by opinions.
●Africanus: black, phlegmatic, relaxed; black, frizzled hair; silky skin, flat nose, tumid lips; females without shame; mammary glands give milk abundantly; crafty, sly, lazy, cunning, lustful, careless; anoints himself with grease; and governed by caprice.
Although these ideas have fallen out of a favor there is a lingering idea that fundamental differences in constitution impact susceptibility to disease.
You can certainly see how we’ve evolved in talking about race and disease. In the nineteenth century, ideas about scientific racism and inherent health differences between races — often used to justify slavery — were firmly entrenched. By the 20th century, though, discourse had shifted to talk about different risk factors for disease, and how these affected groups differently — poverty, housing, education. And now in the 21st century, with COVID-19, discourse has shifted again to talk about how structural racism and bias leads to systemic health inequities.—The Original (Antigenic) Sin—Bedside Rounds
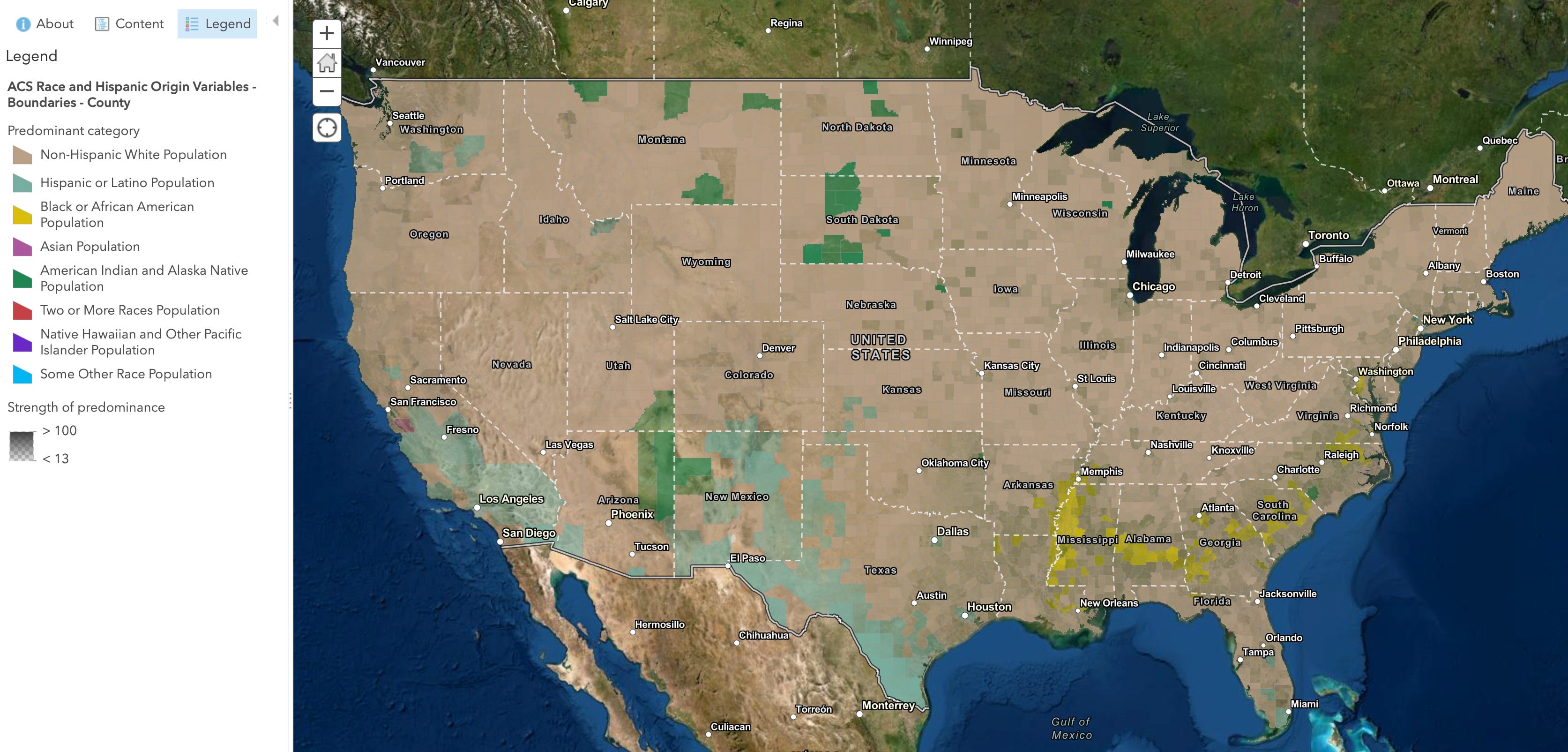
In the new year we will explore CENSUS data looking at how we can define populations by specific risk factors for disease—at higher levels of granularity.